Last updated on May 20, 2026
Get the free HCFA 1500 Medicare Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
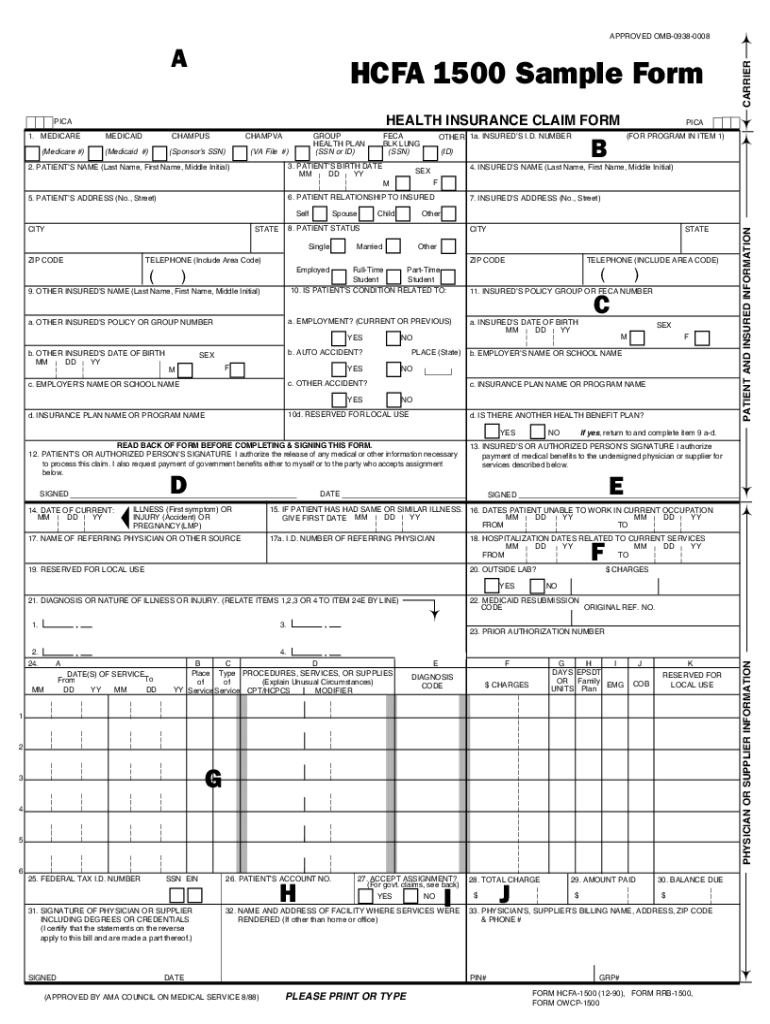
What is HCFA 1500 Medicare Claim Form
The HCFA 1500 Medicare Claim Form is a healthcare document used by providers to bill for services rendered to Medicare beneficiaries.
pdfFiller scores top ratings on review platforms
Pricing is very good
Pricing is very good. Free trial helped a lot to discover vital features. After trial I have decided to purchase a subscription. Esign, editing, and organizing are working perfectly
Very good easy to use program
Very good easy to use program. Customer service is great I miss read and accidentally signed up for a whole year in one go instead of just for the month, they quickly resolved it for me and refunded the difference. =) if I ever need to do documents online again I will definitely use their service again
Who needs HCFA 1500 Medicare Claim Form?
Explore how professionals across industries use pdfFiller.

HCFA 1500 Medicare Claim Form is needed by:
-
Healthcare Providers submitting claims for Medicare services
-
Patients seeking reimbursement for medical expenses
-
Insurance Companies processing Medicare claims
-
Billing Specialists managing healthcare billing processes
-
Healthcare Administrators overseeing Medicare compliance
Comprehensive Guide to HCFA 1500 Medicare Claim Form
What is the HCFA 1500 Medicare Claim Form?
The HCFA 1500 form is a critical document in the healthcare system, primarily used for Medicare billing. This health insurance claim form serves as a means for healthcare providers to submit claims to Medicare and other insurance companies for services rendered to Medicare beneficiaries. The necessity of this form extends to both healthcare providers and patients, ensuring accurate record-keeping and facilitating prompt payment processes.
Healthcare providers rely on the HCFA 1500 form to capture essential patient and service information, which is integral for a smooth billing process. Conversely, patients benefit from the structure the form provides, aiding in transparent communication about their healthcare expenditures.
Purpose and Benefits of the HCFA 1500 Medicare Claim Form
The significance of the HCFA 1500 form lies in its ability to streamline claims submission to Medicare and supplemental insurance companies. This form not only simplifies the process for healthcare providers, ensuring a faster reimbursement cycle, but it also benefits patients by reducing uncertainties regarding their medical claims.
Utilizing the HCFA 1500 for billing helps minimize administrative errors, leading to faster reimbursement timelines and fewer disputes. The structured format of the medicare claim form enhances clarity, making it easier for both patients and providers to track claims and payments.
Key Features of the HCFA 1500 Medicare Claim Form
The HCFA 1500 form contains several key components and fields that must be accurately filled out. Essential information includes patient demographics, insured individual's details, services rendered, and the accompanying signatures required in specific sections.
-
Box 1 requires the patient’s insurance type.
-
Box 13 contains critical "Signature on File" authorization.
-
Detailed descriptions of services and procedures should be noted in their respective fields.
-
The form mandates the inclusion of a tax identification number.
Adhering to any special instructions, particularly in sections like Box 13, is essential for efficient processing.
Who Needs the HCFA 1500 Medicare Claim Form?
-
Healthcare providers including doctors, clinics, and hospitals.
-
Medicare beneficiaries seeking reimbursement for medical services.
-
Patients who have secondary health insurance that may require claim submission.
How to Fill Out the HCFA 1500 Medicare Claim Form Online (Step-by-Step)
Filling out the HCFA 1500 form online can be straightforward with the right tools. Follow these steps to complete the process effectively:
-
Gather all necessary personal information, including insurance details.
-
Access the HCFA 1500 form through a reliable platform like pdfFiller.
-
Fill in patient and provider information precisely.
-
Complete the details of the medical services provided.
-
Verify all information for accuracy before submission.
Having the required documents at hand ensures a hassle-free experience while completing the medicare billing form.
Common Errors and How to Avoid Them When Filing the HCFA 1500 Medicare Claim Form
When filling out the HCFA 1500 form, users frequently encounter common errors that can delay claim processing. To prevent these issues, consider the following strategies:
-
Double-check patient and insurance information for accuracy.
-
Ensure all required fields are filled out and no boxes are left blank.
-
Review any special instructions associated with the form, particularly for Box 13.
-
Use a checklist to validate each section before submitting.
Submission Methods for the HCFA 1500 Medicare Claim Form
The HCFA 1500 form can be submitted through various methods, catering to the preferences of healthcare providers and patients. These include:
-
Electronic submission via Medicare's online portal or third-party services.
-
Traditional mailing to the relevant Medicare administrative contractor.
-
Direct submissions to supplemental insurance companies, when applicable.
Consideration of processing times and delivery confirmations can significantly impact the choice of submission method.
What Happens After You Submit the HCFA 1500 Medicare Claim Form?
After submitting the HCFA 1500 form, several subsequent steps take place. Claimants should track the status of their submission and be aware of the expected processing timelines.
-
Follow up on claim status through the Medicare portal or contact the claims department.
-
Be prepared for potential claim adjustments or denials, which may require additional documentation.
-
Understand the common reasons for claim rejections to address potential issues proactively.
Security and Compliance When Using the HCFA 1500 Medicare Claim Form
Security and confidentiality are paramount when submitting health insurance claims, including the HCFA 1500 form. Users should utilize platforms that prioritize data protection.
pdfFiller employs 256-bit encryption and complies with HIPAA regulations, ensuring sensitive information remains secure throughout the process. It is imperative to choose a platform that adheres to rigorous security standards, protecting your privacy and that of your patients.
Get Started with Filling Out the HCFA 1500 Medicare Claim Form Today
Utilizing pdfFiller can greatly enhance your experience when filling out the HCFA 1500 form. The platform’s user-friendly design supports quick and efficient form completion while maintaining high security standards.
Take advantage of specific features offered by pdfFiller, such as customizable templates and easy electronic signing, to streamline your healthcare claim submission process.
How to fill out the HCFA 1500 Medicare Claim Form
-
1.To access the HCFA 1500 form on pdfFiller, start by logging into your pdfFiller account and searching for 'HCFA 1500 Medicare Claim Form.'
-
2.Once located, click on the form to open it in the editor. Familiarize yourself with the layout and available tools.
-
3.Before starting, gather essential information such as patient details, insurance coverage information, and service specifics.
-
4.Begin completing the form by filling in the patient’s information, including their name, date of birth, and insurance details in the designated fields.
-
5.Next, provide details about the services rendered, including dates of service, procedure codes, and descriptions in the corresponding sections.
-
6.Ensure that both the patient and the insured sign the form where indicated, as signatures are necessary for processing.
-
7.Utilize pdfFiller's tools to check for completeness. Review all text fields and verify that no required information is missing.
-
8.When you are satisfied with the form, click the save option to preserve your changes, and choose the download option to get a copy for your records.
-
9.You can also submit the form directly to your insurance company or Medicare through pdfFiller, selecting the appropriate submission method.

Who is eligible to use the HCFA 1500 form?
The HCFA 1500 form can be used by healthcare providers billing Medicare and insured patients for medical services. Patients receiving services must provide accurate information for submissions.
What documents do I need to complete the HCFA 1500 form?
Before filling out the HCFA 1500 form, gather essential documents such as patient medical records, insurance policy details, and invoices for services rendered to ensure accurate completion.
How can I submit the HCFA 1500 form?
The HCFA 1500 form can be submitted electronically through insurance portals, or you can print the completed form and mail it directly to the insurance or Medicare. Choose the method based on your insurance company’s guidelines.
What are some common mistakes to avoid when completing the HCFA 1500 form?
Common errors include missing required signatures, incorrect procedure codes, and incomplete patient information. Double-check all fields and ensure that both the patient and insured sign the form to avoid delays.
What is the processing time for the HCFA 1500 claims?
Processing times for HCFA 1500 claims vary by insurance provider but typically range from 30 to 90 days. Factors such as claim accuracy and completeness can influence this timeframe.
Is there a fee associated with submitting the HCFA 1500 form?
Generally, there is no fee for submitting the HCFA 1500 form itself, but there may be costs related to the procedures billed. Always verify with your insurance provider for specific fees.
Can I fill out the HCFA 1500 form on my mobile device?
Yes, the HCFA 1500 form can be filled out using mobile devices through pdfFiller. Ensure that you have a stable internet connection for optimal performance.
Related Content
Related Forms






Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.